Orbital Roof Fracture Management

Orbital Roof Fractures A Clinically Based Classification And Treatment Algorithm Omfs

Pdf Early Reconstruction Of Orbital Roof Fractures Clinical Features And Treatment Outcomes Semantic Scholar

Facial Fractures Earwell Center Of Excellence

Pdf Traumatic Orbital Roof Fractures Interdisciplinary Evaluation And Management

Figure 1 From Natural Course Of Orbital Roof Fractures Semantic Scholar

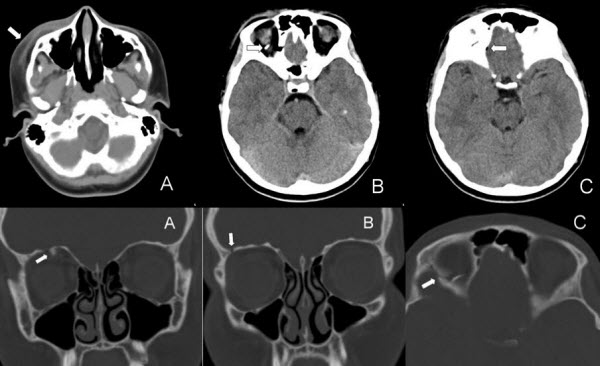
Figure 4 From Reconstruction Of Orbital Roof Fracture Using Titanium Mesh Case Report And Review Of Literature Semantic Scholar
However intracranial or intraorbital injury may warrant surgical intervention to remove impinging bony fragments repair dura or reconstruct the orbital roof.
Orbital roof fracture management.

Diagnosis And Imaging Of Orbital Roof Fractures A Review Of The Current Literature Semantic Scholar
Orbital Roof Blow In Fracture A Case Report And Review Jones Journal Of Radiology Case Reports
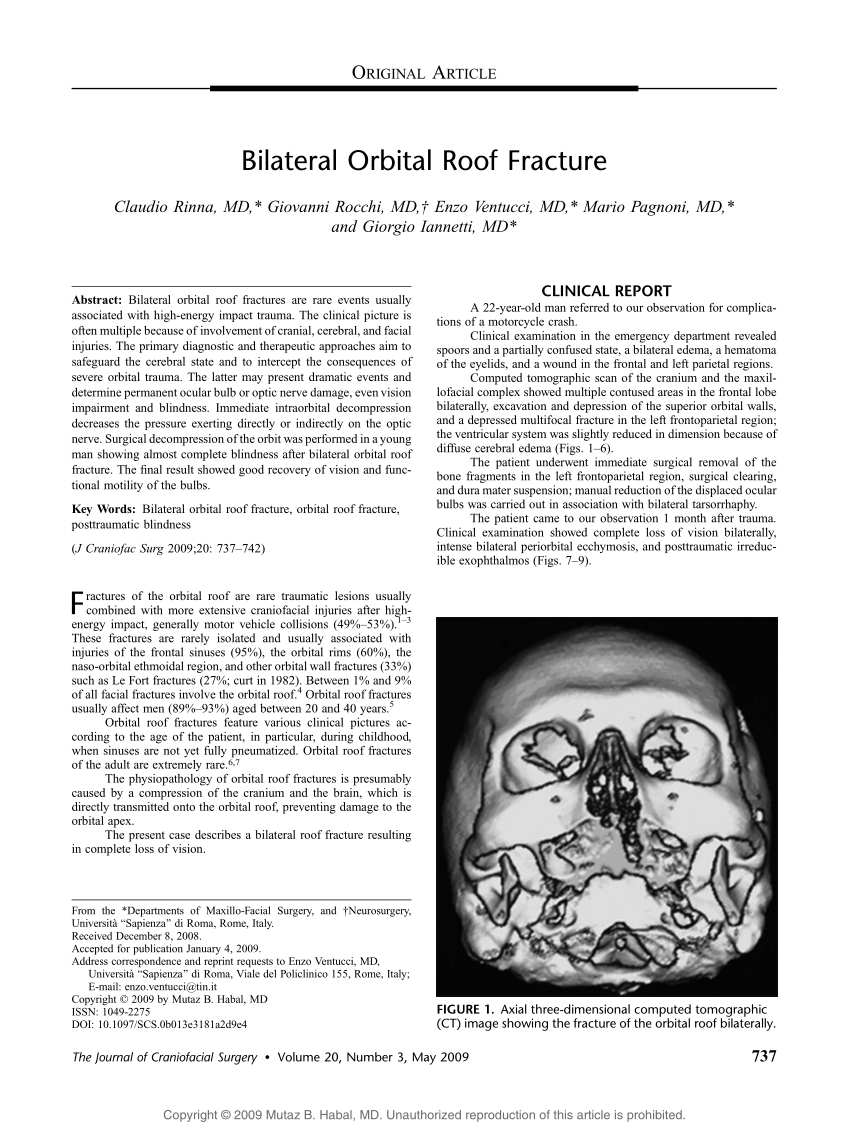
Pdf Bilateral Orbital Roof Fracture

Isolated Orbital Roof Fracture Can It Be Catastrophic Sadashivam S Asian J Neurosurg
Source : pinterest.com
